
https://www.npr.org/sections/goatsandsoda/2023/05/10/1175303067/a-plastic-sheet-with-a-pouch-could-be-a-game-changer-for-maternal-mortality
https://www.bmj.com/content/381/bmj.p1055
I love this study, in and of itself, because it is based on research that will save women's lives without spending a lot of money. I love it.

Here is a link to the original study. I learned about it from an NPR story about the research by Rhitu Chaterjee.
I also love it because it is an accessible example of a bunch of statistics things: Dependent variables...operationalizing variables...why cross-cultural research and solutions aren't just lip service to diversity...how control groups in medical research are very different than control groups in psychology research...absolute vs. relative risk.
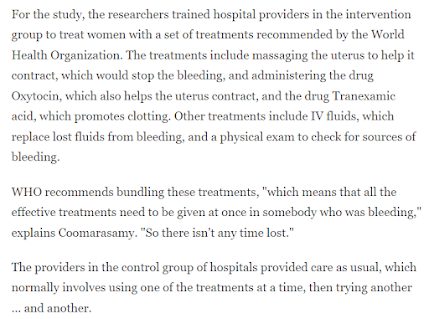
-Dependent variables/operationalized variables: This study clearly illustrates the power of measurement and operationalization. The researchers wanted to create a way to better assess post-childbirth hemorrhaging. Medical professionals created a plastic drape to correctly measure blood loss after pregnancy. The blood loss pools in a plastic pouch, which is far easier to measure than an estimate of blood lost based on blood on the floor, gurney, etc.
 |
| https://www.researchgate.net/figure/Photograph-of-the-calibrated-blood-collection-drape_fig1_281634929 |
-Control group =/= The Nothing Happens Group. In psychology research, the control group usually means nothing is happening. Placebo. However, that is different from what a control group is in medical research. As in many medical research studies, the control group received standard care plus the experimental condition.
 |
| A description of the control group used in this study. |


Also, the interview with the author touches on how research can 1) help explain some but not all of the variance explained, 2) ecological validity, and 3) how real-life interventions are evaluated not just by efficacy/data but by cost and ease of implementation.
